Difference between revisions of "IPLab:Lab 12:Radiation Fibrosis"
(→Clinical Summary) |
(→Autopsy Findings) |
||
| Line 3: | Line 3: | ||
At autopsy there was metastatic carcinoma in the pericardium, chest wall, diaphragm, both lungs, and mediastinal lymph nodes. Areas of pleural thickening with adhesions and interstitial fibrosis were found involving the anterior aspect of both lungs. | At autopsy there was metastatic carcinoma in the pericardium, chest wall, diaphragm, both lungs, and mediastinal lymph nodes. Areas of pleural thickening with adhesions and interstitial fibrosis were found involving the anterior aspect of both lungs. | ||
| − | |||
| − | |||
| − | |||
| − | |||
== Images == | == Images == | ||
Latest revision as of 21:12, 9 July 2020
Contents
Clinical Summary[edit]
This 56-year-old female was diagnosed with breast cancer and underwent a lumpectomy followed by radiation therapy. After 5 years without problems, the patient developed decreased exercise tolerance, dyspnea on exertion, shortness of breath, and an unintentional 15 pound weight loss. Recurrence of the breast cancer was identified but the patient opted for palliative therapy and subsequently expired at home.
At autopsy there was metastatic carcinoma in the pericardium, chest wall, diaphragm, both lungs, and mediastinal lymph nodes. Areas of pleural thickening with adhesions and interstitial fibrosis were found involving the anterior aspect of both lungs.
Images[edit]

This is a gross photograph of lung demonstrating areas of fibrosis on the pleural surface (arrow).
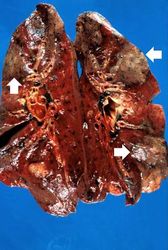
This is a gross photograph of cut sections of lung. There are several areas of fibrosis (arrows) within the lung parenchyma.
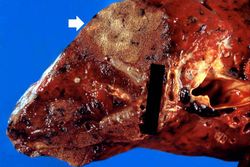
This is a gross photograph showing a closer view of a cut section of lung. An area of fibrosis (arrow) is evident in this photograph.
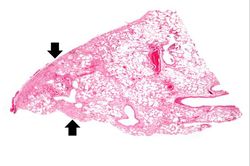
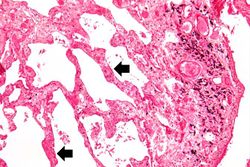
This is a low-power photomicrograph of lung section. Note the thickening of the alveolar septa (arrows).
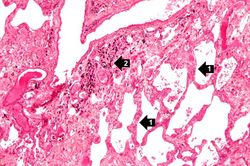
This is a higher-power photomicrograph of lung section. Note the thickening of the alveolar septa (1) and accumulations of anthracotic pigment (2).
This is another high-power photomicrograph of lung section showing the thickening of the alveolar septa (arrows) and accumulations of black anthracotic pigment.
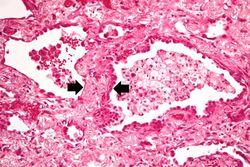
This high-power photomicrograph of lung section shows the thickening of the alveolar septum (arrows) by fibrous connective tissue.
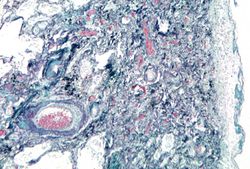
This is a photomicrograph of a trichrome-stained section of lung demonstrating the extensive fibrosis throughout this section (green-blue stained material is fibrous connective tissue).
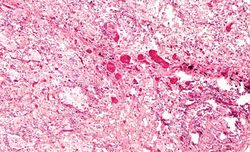
This is a photomicrograph of an area of tissue exhibiting diffuse fibrosis and thickening of the alveolar septa.
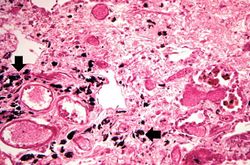
This is another high-power photomicrograph of an area of tissue with diffuse fibrosis and thickening of the alveolar septa. There are also accumulations of anthracotic pigment in this area (arrows).
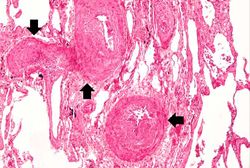
This medium-power photomicrograph shows fibrosis and severe intimal changes in blood vessels (arrows).
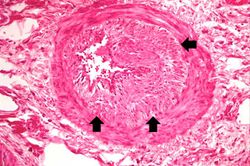
This high-power photomicrograph shows intimal changes (arrows) in this blood vessel in the lung.
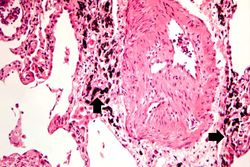
This is a high-power photomicrograph of a recanalized blood vessel in the lung. Notice the anthracotic pigment adjacent to the vessel (arrows).













Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Interstitial (Nonidiopathic) Pulmonary Fibrosis
- Merck Manual: Radiation Exposure and Contamination
Journal Articles[edit]
- White P. Evaluation of pulmonary infiltrates in critically ill patients with cancer and marrow transplant. Crit Care Clin 2001 Jul;17(3):647-70.
Images[edit]
| |||||
Shortness of breath is a common clinical manifestation of heart failure.
Anthracotic pigment is coal dust deposited in the lungs--it is seen in coal miners, city-dwellers, and smokers.
Recanalization is the process of the forming of channels through an organized thrombus so that blood flow is restored.
Pulmonary congestion is the engorgement of pulmonary vessels with blood. The increased pressure caused by this engorgement leads to transudation of fluid through the capillary walls and into the alveolar and interstitial spaces.
Respiratory distress syndrome (or hyaline membrane disease) is a common complication of prematurity, though it can also be seen in term births. The syndrome results from the functional immaturity of the neonatal lung. The syndrome usually presents within one hour of birth and is initially exhibited clinically by rapid respirations, grunting, and substernal retractions.