Difference between revisions of "IPLab:Lab 12:Alcoholic Cirrhosis"
Seung Park (talk | contribs) (→Journal Articles) |
(→Clinical Summary) |
||
| (5 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| + | This 56-year-old white male came to the emergency room because of weakness, lack of appetite, shortness of breath, abdominal distention, and an altered mental status. He was a known to have alcohol use disorder and he drank approximately one pint of whiskey per day. Physical examination revealed a protuberant abdomen, bilateral gynecomastia, and spider angiomata on his chest. Liver enzymes were elevated, albumin was low and he was anemic. | ||
| − | + | The patient was given thiamine, folate, multivitamins, and vitamin K and an intravenous line was placed to infuse 5% dextrose. An esophagogastroduodenoscopy (EGD) demonstrated large esophageal varices. Two days after admission the patient developed a massive hematemesis due to rupture of an esophageal varices and despite successful sclerotherapy and supportive transfusions, the patient died the next day. | |
== Images == | == Images == | ||
| Line 43: | Line 44: | ||
=== Journal Articles === | === Journal Articles === | ||
* Fujimoto J. [http://www.ncbi.nlm.nih.gov/pubmed/10759218 Gene therapy for liver cirrhosis]. ''J Gastroenterol Hepatol'' 2000 Mar;15 Suppl:D33-6. | * Fujimoto J. [http://www.ncbi.nlm.nih.gov/pubmed/10759218 Gene therapy for liver cirrhosis]. ''J Gastroenterol Hepatol'' 2000 Mar;15 Suppl:D33-6. | ||
| + | * Ge PS and Runyon BA [http://www.nejm.org/doi/pdf/10.1056/NEJMra1504367 Treatment of Patients with Cirrhosis]. ''NEJM'' 2016 Aug 25 375(8):767. | ||
=== Images === | === Images === | ||
| − | + | * [{{SERVER}}/library/index.php?/tags/128-cirrhosis PEIR Digital Library: Cirrhosis Images] | |
| + | * [http://library.med.utah.edu/WebPath/LIVEHTML/LIVERIDX.html WebPath: Hepatic Pathology] | ||
== Related IPLab Cases == | == Related IPLab Cases == | ||
| − | + | * [[IPLab:Lab 2:Fatty Change and Cirrhosis|Lab 2: Liver: Fatty Change and Cirrhosis]] | |
{{IPLab 12}} | {{IPLab 12}} | ||
[[Category: IPLab:Lab 12]] | [[Category: IPLab:Lab 12]] | ||
Latest revision as of 21:10, 9 July 2020
Contents
Clinical Summary[edit]
This 56-year-old white male came to the emergency room because of weakness, lack of appetite, shortness of breath, abdominal distention, and an altered mental status. He was a known to have alcohol use disorder and he drank approximately one pint of whiskey per day. Physical examination revealed a protuberant abdomen, bilateral gynecomastia, and spider angiomata on his chest. Liver enzymes were elevated, albumin was low and he was anemic.
The patient was given thiamine, folate, multivitamins, and vitamin K and an intravenous line was placed to infuse 5% dextrose. An esophagogastroduodenoscopy (EGD) demonstrated large esophageal varices. Two days after admission the patient developed a massive hematemesis due to rupture of an esophageal varices and despite successful sclerotherapy and supportive transfusions, the patient died the next day.
Images[edit]

This is a gross photograph of the liver from this patient. Note the nodular pattern and the areas of greenish discoloration as well as pale tan areas.

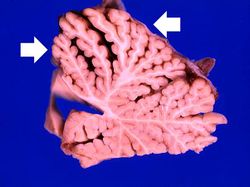
This is a closer view of the liver from this patient. Again note the nodular pattern and the areas of greenish discoloration. These green nodules are actually the viable hepatocytes that are stained green because of bile stasis. The pale areas are the areas of fibrosis.
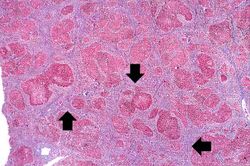
This is a low-power photomicrograph of this liver stained with a trichrome stain to highlight the fibrous tissue (arrows). Also note the nodular pattern.
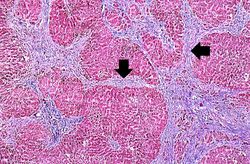
In this is medium-power photomicrograph of trichrome stained liver the bands of fibrous tissue are seen to form "bridges" between triad areas (arrows); this is called "bridging fibrosis." Also note the fibrous tissue (arrows) and how the hepatocytes are separated into nodules by this fibrous tissue.
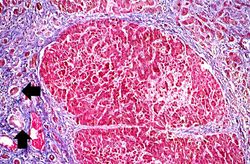
In this high-power photomicrograph of trichrome-stained liver, the bands of fibrous tissue surround the hepatocyte nodules. There is some degeneration and dropout of hepatocytes in this nodule. Also note the increased numbers of bile ducts in the triad area (arrows). Bile duct proliferation is a common feature in many hepatitides.

This photograph from another autopsy case shows another example of cirrhosis. Note the nodules, the fibrosis, the green coloration and the small size of this cirrhotic liver.
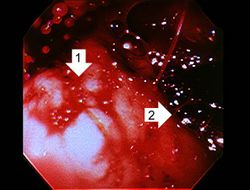
This photograph was taken during the EGD while the patient was alive. Note the red hyperemic areas (1) and the area of hemorrhage (2).
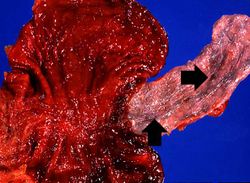
This photograph taken at autopsy shows the distal portion of the esophagus and the stomach. The esophageal varices are visible just under the mucosa of the esophagus (arrows). Some of the blood from the ruptured varix can still be seen in the stomach.

In this closer view of the distal esophagus the ruptured varix is indicated by the probe. Other varices and areas of submucosal hemorrhage can also be appreciated.
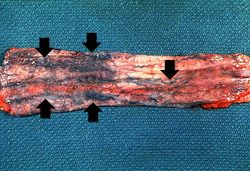
This is a photograph taken from another patient at autopsy to demonstrate numerous esophageal varices in the distal esophagus (arrows). None of these varices have ruptured.
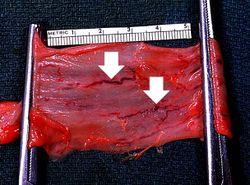
This photograph taken from still another patient at autopsy demonstrates the esophageal varices in the distal esophagus (arrows). The esophagus was clamped before removing the esophagus from the body in order to trap the blood in these distended varices. It is obvious how easily these thin-walled superficial varices could rupture and bleed.
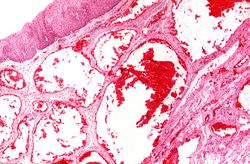
This photomicrograph shows the dilated vessel just under the epithelium of the esophagus.

This photograph of the cerebellum from this patient demonstrates the marked thinning of the anterior portion of the cerebellum (arrows).
This is another photograph of the cerebellum from this patient demonstrating the marked thinning of the anterior portion of the cerebellum (arrows). This pattern of cerebellar damage is consistent with Wernicke's encephalopathy.














Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Cirrhosis
- eMedicine Medical Library: Cirrhosis Imaging
- Merck Manual: Alcoholic Liver Disease
Journal Articles[edit]
- Fujimoto J. Gene therapy for liver cirrhosis. J Gastroenterol Hepatol 2000 Mar;15 Suppl:D33-6.
- Ge PS and Runyon BA Treatment of Patients with Cirrhosis. NEJM 2016 Aug 25 375(8):767.
Images[edit]
Related IPLab Cases[edit]
| |||||
Shortness of breath is a common clinical manifestation of heart failure.
A focal network of small arteries and arterioles arranged in a radial pattern with a central red spot.
Hematemesis is the vomiting of blood.
Nodular hyperplasia of the prostate--characterized by large discrete prostatic nodules--is a common disorder in men over 50 years of age. The nodules cause the prostate to be enlarged and to have an increased weight. The human prostate is surrounded by a restrictive capsule. These nodules cause increased pressure within the capsule which leads to constriction of the urethra as it passes through the prostate. Urethral constriction leads to retention of urine.
Cirrhosis is a liver disease characterized by necrosis, fibrosis, loss of normal liver architecture, and hyperplastic nodules.