IPLab:Lab 10:Cryptococcosis
Contents
Clinical Summary[edit]
This 46-year-old male presented with a complaint of right-sided chest pain of six months duration. Chest x-ray showed a nodular mass in the lower lobe of the right lung. The mass was resected surgically.
The 3.5 x 2.5-cm mass was firm, gray, and gelatinous. The mass proved to be a cryptococcal lesion.
Images[edit]

This is the chest x-ray showing the mass (arrow) in the right lower lobe.
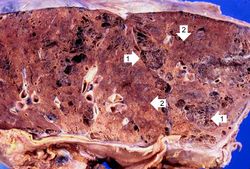
This is a gross photomicrograph of this lung taken at autopsy. Note the areas of emphysema (1) and consolidation (2).

This is another section of this lung showing consolidation (arrows).

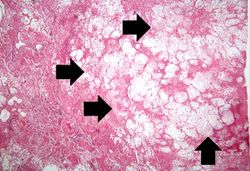
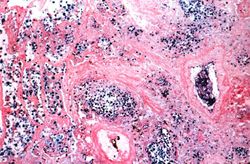
This is a low-power photomicrograph of the lung from the lesion seen on x-ray. Note that there is little, if any, inflammatory reaction.
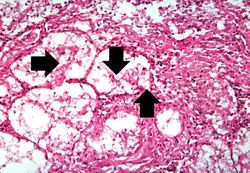
This is a higher-power photomicrograph of the cryptococcal lesion. The air spaces are filled with organisms (arrows).
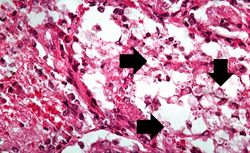
This is a high-power photomicrograph of the cryptococcal lesion. Some of the organisms have been expelled during processing, but some cryptococcal organisms can be seen (arrows).
This is another high-power photomicrograph of the cryptococcal lesion. In this section, numerous cryptococcal organisms (5-10 mm in diameter) can be seen (arrows). Note that there is very little inflammatory reaction.
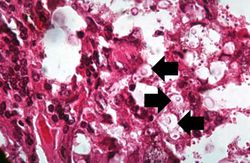
Cryptococcal organisms can also be seen in this high-power photomicrograph of the cryptococcal lesion. Some of the organisms have a well-defined halo (arrows) due to the mucopolysaccharide coat which surrounds them.
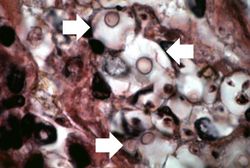
This higher-power photomicrograph of a cryptococcal organism shows more clearly the nucleus surrounded by the large extracellular capsule (arrows).
This is a low-power photomicrograph of lung section stained with Alcian blue, which stains the acidic glycosaminoglycans making up the coat of the cryptococcal organism.
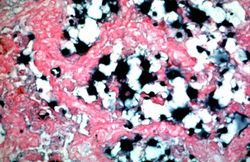
This is a higher-power photomicrograph of lung section stained with Alcian blue. The mucopolysaccharide capsule shrinks during processing with this stain, thereby producing a shrunken central appearance with the formation of spikes around each organism.
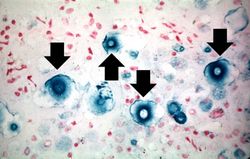
This is a touch prep of fresh lung tissue that was allowed to air dry and then stained to show the mucopolysaccharide capsule around the cryptococcal organisms (arrows).












Virtual Microscopy[edit]
H&E[edit]
Mucicarmine[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- Rooney PJ, Klein BS. Linking fungal morphogenesis with virulence. Cell Microbiol 2002 Mar;4(3):127-37.
Images[edit]
Related IPLab Cases[edit]
| |||||
Nodular hyperplasia of the prostate--characterized by large discrete prostatic nodules--is a common disorder in men over 50 years of age. The nodules cause the prostate to be enlarged and to have an increased weight. The human prostate is surrounded by a restrictive capsule. These nodules cause increased pressure within the capsule which leads to constriction of the urethra as it passes through the prostate. Urethral constriction leads to retention of urine.
Pulmonary emphysema is a condition in which the air spaces distal to the terminal bronchioles are permanently increased in size due to either destruction of the wall or alveolar dilatation.