IPLab:Lab 7:Adenocarcinoma
Contents
Clinical Summary[edit]
Approximately four months prior to admission, this 68-year-old male began having "sharp, shooting pains" in the lower abdomen. A barium enema at that time was reported as normal. Two months later, the barium study was repeated because of persistent diarrhea and showed a filling defect in the transverse colon. The patient refused to undergo an exploratory laparotomy. During the week prior to this admission, the patient had recurrent diarrhea, cramping abdominal pain, and marked rectal bleeding. He was hospitalized and required 2500 ml of blood to return his hematocrit to normal. A colectomy was done from the hepatic flexure to the rectosigmoid.
Autopsy Findings[edit]
The segment of colon contained numerous polyps and an annular tumor which was 6.7 cm in diameter. Proctoscopic examination of the ascending colon revealed two more polyps which were removed.
Images[edit]
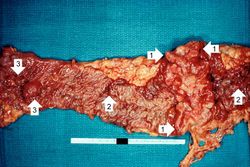
This is a gross photograph of the adenoma from the surgical specimen in this case. Note the large, ulcerated, fungating annular (encircling) carcinoma (1) with areas of hemorrhage (2). Also note the adenomatous polyps (3).

This is a closer view of the previous image demonstrating the raised, annular carcinoma (arrows).
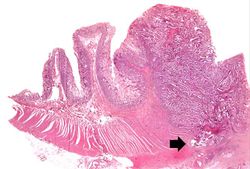
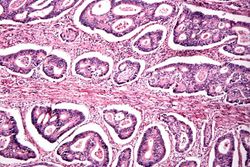
This photomicrograph of the surgical specimen shows the transition between normal mucosa on the left and carcinoma which is invading the wall of the bowel (arrow).
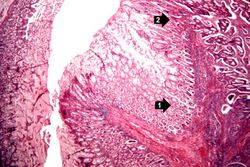
This is a higher-power photomicrograph of the area of transition between the normal (1) and the neoplastic (2) epithelium.
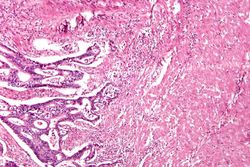
This is a high-power photomicrograph of tumor cells invading the underlying muscularis.
This is a high-power photomicrograph of tumor cells forming glands.
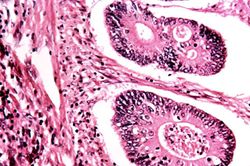
This is a high-power photomicrograph of tumor cells forming glands.

This gross photograph from another case demonstrates an ulcerated adenocarcinoma (arrows) at the rectosigmoid junction.

This is a segment of distal colon from another case. Note the annular tumor that severely compromises the lumen of the colon. There is dilation of the colon proximal to the tumor.









Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
Images[edit]
Related IPLab Cases[edit]
A barium enema is a radiological study of the colon and rectum performed using barium as a contrast agent.
Any localized defect in the contour of the stomach, duodenum, or intestine, as seen in the radiograph after a barium enema.
Melena is the passage of digested blood in the feces.