IPLab:Lab 5:Polycystic Kidney Disease
Clinical Summary[edit]
This 64-year-old white man had a history of hypertension, adult-onset diabetes, gouty arthritis, chronic obstructive pulmonary disease (COPD), chronic anemia, bleeding from colonic polyps, and bleeding from gastric ulcers. The patient was in end-stage renal failure due to polycystic kidney disease and he required renal dialysis. His mother and a brother both died from renal complications.
His terminal admission was for congestive heart failure and ventricular tachycardia. He underwent a coronary artery bypass grafting (CABG) operation after which he was ventilator-dependent. Two days after the operation he developed pneumonia and died.
Autopsy Findings[edit]
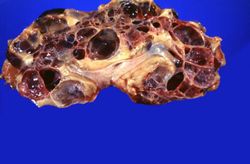
The lungs were diffusely consolidated with some abscesses in the right upper lobe. The kidneys were markedly enlarged. The right kidney weighed 1660 grams and the left kidney weighted 1780 grams.
Images[edit]

This is a gross photograph of the kidneys from this case. Note that both kidneys contain multiple large cysts (arrows).

This is a gross photograph of one of the kidneys from this case next to a normal kidney. This photograph demonstrates how big these polycystic kidneys are compared to a normal kidney.
This is a gross photograph of a cut section from one of these polycystic kidneys. Note that the renal parenchyma is almost completely replaced by cystic structures.
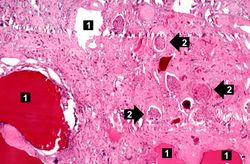
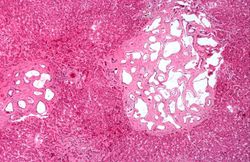
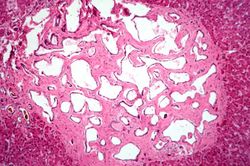
This is a low-power photomicrograph of an H&E-stained section from this polycystic kidney. Note the large cystic structures (1), the few residual glomeruli (2), and the fibrous connective tissue throughout this section.
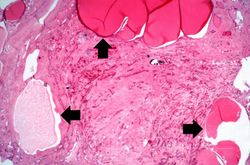
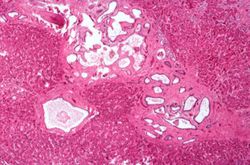
This is another low-power photomicrograph of an H&E-stained section from this polycystic kidney. Again note the large cystic structures (arrows)and the fibrous connective tissue throughout this section.
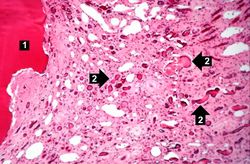
This is a higher-power photomicrograph of polycystic kidney showing the edge of a large cyst (1). In this section there are numerous tubules and dilated collecting ducts (2) that are filled with the same red proteinaceous material as the larger cysts.
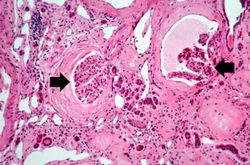
This high-power photomicrograph shows abnormal glomeruli (arrows) and some tubules.
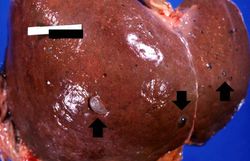
This is a gross photograph of the liver from this patient. Multiple cysts can be seen on the surface of this liver (arrows).
This photomicrograph of liver demonstrates the histologic appearance of these cysts.
This is another photomicrograph of liver demonstrating the histologic appearance of these cysts. These cystic structures are associated with the biliary tree.
This is a higher-power photomicrograph of liver cyst. These cystic structures are lined by biliary epithelium.











Study Questions[edit]
| |||||
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
Consolidation is the filling of lung air spaces with exudate--this is a sign of pneumonia.
An abscess is a collection of pus (white blood cells) within a cavity formed by disintegrated tissue.
A normal kidney weighs 157 grams (range: 115 to 220 grams).
A normal kidney weighs 157 grams (range: 115 to 220 grams).
Pericarditis is inflammation of the pericardium - often with deposition of fibrin.