IPLab:Lab 7:Bronchogenic Carcinoma
Clinical Summary[edit]
This 55-year-old white male had a long history of emphysema and a 60-70 pack-year smoking history. He was in his usual state of health until about one month before admission, at which time he developed increasing dyspnea on exertion. At the same time, his sputum increased from two tablespoons to half a cup of yellow blood-streaked sputum a day. Chest x-ray showed a right hilar mass. Sputum cytology revealed abnormal cells that were "positive for malignancy." He later developed pneumonia and fever. The patient expired soon thereafter.
Autopsy Findings[edit]
Significant findings included advanced carcinoma of the right main stem bronchus with extension across the carina to produce obstruction of the left main stem bronchus. There was left lower lobe pneumonia and left upper lobe atelectasis. Extensive metastases were present in regional lymph nodes as well as the pericardium, left atrium, and right kidney.
Images[edit]
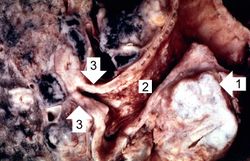
This is a gross photograph of bronchogenic carcinoma. The large tumor mass can be seen adjacent to the bronchus (1). Note that the epithelial surface of the bronchus is rough and irregular (2). The first branch off the right main stem bronchus is partially occluded by the thickened mucosa and submucosa (3).
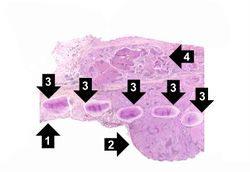
This is a low-power photomicrograph of bronchus showing normal mucosa (1) with transition to carcinoma (2). Note the bronchial cartilage (3) and the invasion of tumor through the entire wall of the bronchus with tumor extending to the serosal surface (4).
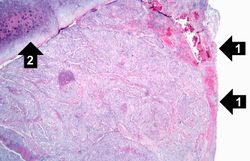
This is a photomicrograph of bronchus with ulcerated mucosal surface on the right (1). The submucosa is completely filled with tumor down to the cartilage (2).
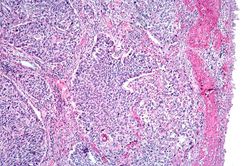
This is a higher-power photomicrograph of bronchus with the ulcerated mucosal surface on the right and tumor underneath.
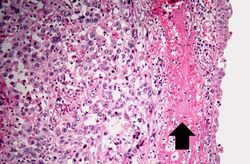
This is a higher-power photomicrograph of the mucosal surface (right) with an area of hemorrhage (arrow) and underlying tumor (left).
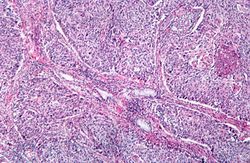
This is a photomicrograph of tumor from an area of invasion with compression of fibrous stroma and focal necrosis.
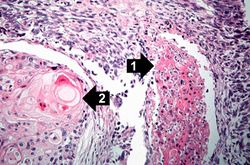
This is a high-power photomicrograph showing cytologic detail of the tumor with an area of necrosis (1) and a more differentiated area with keratin pearl formation (2).
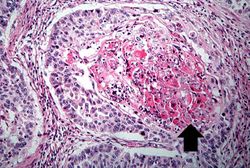
This is a high power photomicrograph of tumor with an area of central necrosis (arrow).
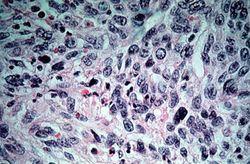
This high-power photomicrograph of tumor shows the cytologic detail of a less-differentiated area of neoplasm with cellular anaplasia.









Pulmonary emphysema is a condition in which the air spaces distal to the terminal bronchioles are permanently increased in size due to either destruction of the wall or alveolar dilatation.
A pack-year denotes smoking one pack of cigarettes per day for one year.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
Atelectasis is the collapse of an airway and lung, regardless of the cause, resulting in reduced or absent gas exchange.