IPLab:Lab 6:PAN
Clinical Summary[edit]
This was a 27-year-old white female who presented to the emergency room with fever, diarrhea, and abdominal pain that had increased in intensity over a 3-day period. Her blood pressure on admission was 165/108 mm Hg. She had been diagnosed with polyarteritis nodosa two years prior to this admission and had been treated with corticosteroids and cyclophosphamide. She had discontinued her corticosteroids because they made her gain weight; in addition, she was not taking the medications prescribed for her hypertension. At this admission it was suspected that the patient had bowel ischemia due to mesenteric artery occlusion. Angiographic evaluation revealed significant vascular damage to the mesenteric arteries with aneurysmal dilatations and thromboses. Significant vascular changes were also observed in the renal and hepatic circulation. On the second hospital day, the patient developed acute severe abdominal pain and an emergency laparotomy was performed to resect an 18-cm section of infarcted and ruptured ileum. After surgery she continued to run a fever, her white blood cell count was 13,500 cells/cmm, and she developed renal failure. Two days after surgery the patient died due to sepsis and multisystem failure.
Autopsy Findings[edit]
At autopsy there were several 0.5 to 1.0-cm firm nodules in the dermis. There were numerous aneurysmal dilatations grossly visible in the mesenteric arteries. There were multiple shrunken infarcts on the surface of the kidneys and the surface also had a fine granular appearance indicative of hypertensive renal disease. On cut section both the kidney and the liver had multiple firm white nodules.
Images[edit]
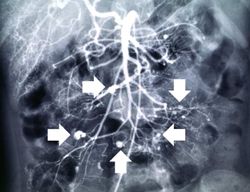
This angiogram of the abdominal viscera demonstrates numerous aneurysms throughout the mesenteric circulation (arrows).

This angiogram of the liver also demonstrates numerous aneurysms throughout the hepatic circulation (arrows).

This angiogram of the kidneys demonstrates numerous aneurysmal dilatations in the renal circulation (arrows).
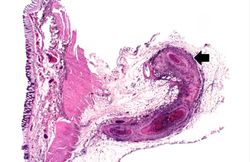
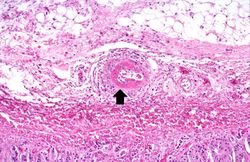
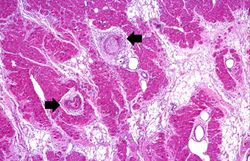
This is a low-power photomicrograph of a mesenteric vessel from this case of polyarteritis nodosa (arrow). The vessel is completely occluded by thrombotic material and the vessel wall is infiltrated with inflammatory cells.
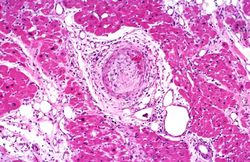
This is a higher-power photomicrograph of this mesenteric vessel. Note the thrombotic material occluding the vessel (arrows) and the inflammatory cell infiltrate in the wall of the vessel and in the surrounding adventitia.
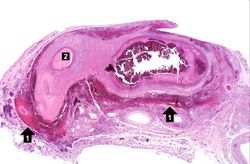
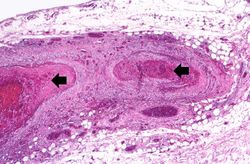
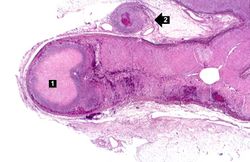
his is another example of a mesenteric artery from this case. There is a marked inflammatory cell response surrounding this vessel, fresh hemorrhage (1), and thrombotic material (2).

This is a high-power photomicrograph of the vessel wall. There is hemorrhage and infiltration with inflammatory cells--primarily neutrophils (arrows).
This is a high-power photomicrograph of a small vessel with a rim of fibrinoid necrosis (arrow).
This is a low-power photomicrograph of the adrenal gland. There is an area of necrosis in the adrenal (1) and an affected vessel adjacent to the adrenal (2).
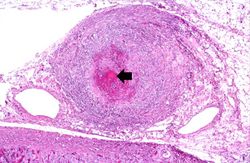
This is a higher-power photomicrograph of the affected vessel from the previous image. The vessel wall is infiltrated with inflammatory cells and the vessel lumen is completely occluded (arrow).
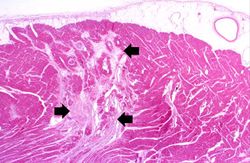
This is a low-power photomicrograph of the heart. There are areas of fibrosis in the myocardium (arrows). Note that the large epicardial coronary artery is normal.
This is a higher-power photomicrograph of the affected vessels in the heart (arrows). There are areas of fibrosis (old infarcts) in the myocardium adjacent to these affected vessels.
This is a high-power photomicrograph of the affected vessel in the heart. The vessel lumen is completely occluded.













Study Questions[edit]
A normal blood pressure reading would be 120/80 mm Hg.
An occlusion is a blockage.
Renal failure is the severe reduction of renal function and often leads to reduced urinary output.
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.
The normal fibrinogen level is 184 to 412 mg/dL.