IPLab:Lab 10:Histoplasmosis
Contents
Clinical Summary[edit]
For four months before death, this two-year-old black female infant ate poorly and lost weight. When hospitalized, she appeared chronically ill with signs of infection. An exploratory laparotomy showed the patient had enormously enlarged abdominal lymph nodes, the biopsy of which disclosed active histoplasmosis. Despite intensive therapy, the patient died three weeks after admission.
Autopsy Findings[edit]
Autopsy showed widespread enlargement of lymph nodes, ulcers of the intestines, and enlarged adrenal glands exhibiting multifocal granulomas.
Images[edit]

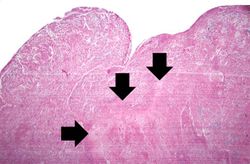
This low-power photomicrograph shows a section of adrenal gland with several irregularly-outlined areas of necrosis.
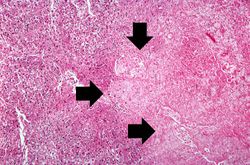
This higher-power photomicrograph of the previous adrenal gland shows more clearly the irregularly-shaped area of necrosis (arrows).
This is an even higher-power photomicrograph of an area of necrosis (arrows). There is loss of cellular detail within this area. There are inflammatory cells present; however, it is difficult to differentiate the inflammatory cells from the native lymphocytes of the adrenal gland--which is a lymph node.
This high-power photomicrograph was taken at the edge of the area of necrosis. There is a mild inflammatory infiltrate along the edge of the necrosis.
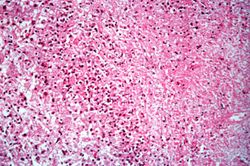
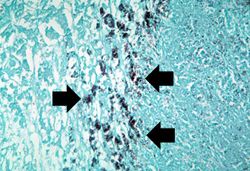
This high-power photomicrograph shows small (2-5 mm) dark-staining organisms in the cytoplasm of many of these cells (arrows).
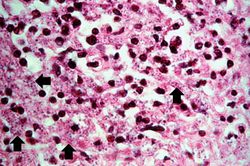
This is a high-power photomicrograph of the same section of tissue as the previous slide. This section, however, has been stained with methenamine silver which causes the Histoplasma organisms to stain black (arrows).
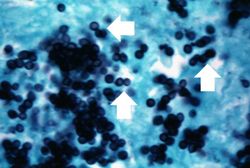
This photomicrograph was taken under oil immersion to show the silver-stained Histoplasma organisms. Some of the organisms appear to be budding (arrows).







Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- de Pauw BE. Advances in the management of invasive fungal infections in organ transplant recipients: step by step. Transpl Infect Dis 2000 Jun;2(2):48-50.
Images[edit]
| |||||
An infiltrate is an accumulation of cells in the lung parenchyma--this is a sign of pneumonia.