Difference between revisions of "IPLab:Lab 2:Fatty Change and Cirrhosis"
Seung Park (talk | contribs) (→Related IPLab Cases) |
(→Images) |
||
| (10 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
== Clinical Summary == | == Clinical Summary == | ||
| − | This 54-year-old man with a long history of alcohol abuse | + | This 54-year-old man with a long history of alcohol abuse disorder. Three weeks prior to his demise, the patient began an alcoholic binge. Three days prior to admission the patient developed fever and malaise and when he was brought to the hospital he was semi-comatose and had a fever of 104.5°F. Shortly after arriving at the hospital, the patient died from massive pneumonia. |
| − | + | At autopsy, a necrotizing lobar pneumonia was present which contained organisms consistent with Klebsiella pneumoniae. The liver was enlarged--weighing 2700 grams--and had a yellow-orange color. The liver was firm to palpation and the cut surface had a slightly granular appearance suggestive of early cirrhosis. The pancreas showed multiple areas of fibrosis. | |
| − | At autopsy, a necrotizing lobar pneumonia was present which contained organisms consistent with Klebsiella pneumoniae. The liver was enlarged--weighing 2700 grams--and had a yellow-orange color. The liver was firm to palpation and the cut surface had a slightly granular appearance suggestive of early cirrhosis. The pancreas showed multiple areas of fibrosis. | ||
== Images == | == Images == | ||
| Line 9: | Line 8: | ||
File:IPLab2FattyChange1.jpg|This gross photograph of liver tissue illustrates the yellowish color of the liver parenchyma. The yellow color indicates high fat content in this tissue. Compare this with the normal dark red color of liver. | File:IPLab2FattyChange1.jpg|This gross photograph of liver tissue illustrates the yellowish color of the liver parenchyma. The yellow color indicates high fat content in this tissue. Compare this with the normal dark red color of liver. | ||
File:IPLab2FattyChange2.jpg|This low-power photomicrograph of liver illustrates a very pale-staining section with a uniform appearance throughout the section. | File:IPLab2FattyChange2.jpg|This low-power photomicrograph of liver illustrates a very pale-staining section with a uniform appearance throughout the section. | ||
| − | File: | + | File:IPLab2FattyChange3b.jpg|Another low-power photomicrograph illustrates again the pale, washed-out appearance of this tissue. Notice the numerous holes throughout the tissue. There are accumulations of inflammatory cells (arrow) around portal tracts. |
| − | File: | + | File:IPLab2FattyChange4b.jpg|A higher-power photomicrograph illustrates more clearly the inflammatory cells (arrow) around the portal areas. |
| − | File: | + | File:IPLab2FattyChange5b.jpg|High power view of hepatocytes with lipid vacuoles. In many cases the nucleus is displaced to the periphery of the cell and the entire cytoplasm is taken up by the giant lipid vacuole. |
| − | |||
| − | |||
File:IPLab2FattyChange8.jpg|An oil red O stain for fat was performed on a frozen section of this liver tissue. The red droplets represent fat in the tissue which is typical of fatty degeneration in the liver. By using frozen sections the tissues do not have to be dehydrated through alcohol solutions and thus the fat does not get washed out. | File:IPLab2FattyChange8.jpg|An oil red O stain for fat was performed on a frozen section of this liver tissue. The red droplets represent fat in the tissue which is typical of fatty degeneration in the liver. By using frozen sections the tissues do not have to be dehydrated through alcohol solutions and thus the fat does not get washed out. | ||
| − | File:IPLab2FattyChange9.jpg|This photomicrograph of the liver is from another patient with a history of alcohol use. There are some clear vacuoles indicating fat droplets (1) and there are numerous red-staining granular deposits within the cytoplasm of hepatocytes ( | + | File:IPLab2FattyChange9.jpg|This photomicrograph of the liver is from another patient with a history of alcohol use. There are some clear vacuoles indicating fat droplets (1) and there are numerous red-staining granular deposits within the cytoplasm of hepatocytes (3)this is alcoholic hyalin. Alcoholic hyalin is easily distinguished from red blood cells (2) that are also present in this section. |
| − | File: | + | File:IPLab2FattyChange10b.jpg|This is a low-power photomicrograph of liver stained with a trichrome stain. In this section, connective tissue stains blue (arrows) and hepatic parenchymal cells are red. Note that many of the parenchymal cells have clear spaces indicating fatty degeneration. The proliferation of scar tissue between the liver lobules is the result of cirrhosis. |
File:IPLab2FattyChange11.jpg|This gross photograph of liver demonstrates severe nodular cirrhosis. Note the extensive scarring of the capsule and the nodular projections of tissue through the uncut capsule in this tissue. The green color is due to the accumulation of bile pigment. | File:IPLab2FattyChange11.jpg|This gross photograph of liver demonstrates severe nodular cirrhosis. Note the extensive scarring of the capsule and the nodular projections of tissue through the uncut capsule in this tissue. The green color is due to the accumulation of bile pigment. | ||
File:IPLab2FattyChange12.jpg|This is a cut surface of the same tissue seen in the previous slide. Note the marked nodular pattern. The paler-staining areas between the round nodules represent fibrous connective tissue. | File:IPLab2FattyChange12.jpg|This is a cut surface of the same tissue seen in the previous slide. Note the marked nodular pattern. The paler-staining areas between the round nodules represent fibrous connective tissue. | ||
| + | </gallery> | ||
| − | </ | + | == Virtual Microscopy == |
| + | === Liver: Fatty Change and Cirrhosis === | ||
| + | <peir-vm>IPLab2FattyChange</peir-vm> | ||
| + | |||
| + | === Normal Liver === | ||
| + | <peir-vm>UAB-Histology-00149</peir-vm> | ||
== Study Questions == | == Study Questions == | ||
| Line 56: | Line 59: | ||
=== Images === | === Images === | ||
| − | * [ | + | * [{{SERVER}}/library/index.php?/tags/128-cirrhosis PEIR Digital Library: Cirrhosis Images] |
| − | * [ | + | * [{{SERVER}}/library/index.php?/tags/231-fatty_change PEIR Digital Library: Fatty Change Images] |
* [http://library.med.utah.edu/WebPath/LIVEHTML/LIVERIDX.html#2 WebPath: Cirrhosis] | * [http://library.med.utah.edu/WebPath/LIVEHTML/LIVERIDX.html#2 WebPath: Cirrhosis] | ||
Latest revision as of 20:56, 19 June 2020
Contents
Clinical Summary[edit]
This 54-year-old man with a long history of alcohol abuse disorder. Three weeks prior to his demise, the patient began an alcoholic binge. Three days prior to admission the patient developed fever and malaise and when he was brought to the hospital he was semi-comatose and had a fever of 104.5°F. Shortly after arriving at the hospital, the patient died from massive pneumonia.
At autopsy, a necrotizing lobar pneumonia was present which contained organisms consistent with Klebsiella pneumoniae. The liver was enlarged--weighing 2700 grams--and had a yellow-orange color. The liver was firm to palpation and the cut surface had a slightly granular appearance suggestive of early cirrhosis. The pancreas showed multiple areas of fibrosis.
Images[edit]
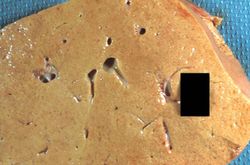
This gross photograph of liver tissue illustrates the yellowish color of the liver parenchyma. The yellow color indicates high fat content in this tissue. Compare this with the normal dark red color of liver.

This low-power photomicrograph of liver illustrates a very pale-staining section with a uniform appearance throughout the section.
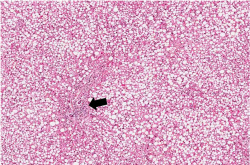
Another low-power photomicrograph illustrates again the pale, washed-out appearance of this tissue. Notice the numerous holes throughout the tissue. There are accumulations of inflammatory cells (arrow) around portal tracts.
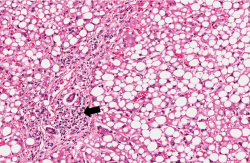
A higher-power photomicrograph illustrates more clearly the inflammatory cells (arrow) around the portal areas.
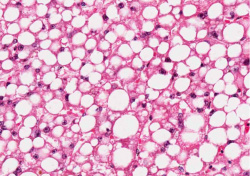
High power view of hepatocytes with lipid vacuoles. In many cases the nucleus is displaced to the periphery of the cell and the entire cytoplasm is taken up by the giant lipid vacuole.
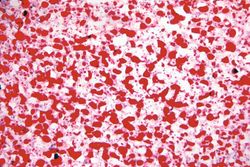
An oil red O stain for fat was performed on a frozen section of this liver tissue. The red droplets represent fat in the tissue which is typical of fatty degeneration in the liver. By using frozen sections the tissues do not have to be dehydrated through alcohol solutions and thus the fat does not get washed out.
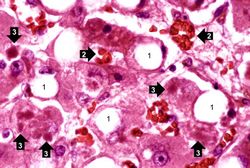
This photomicrograph of the liver is from another patient with a history of alcohol use. There are some clear vacuoles indicating fat droplets (1) and there are numerous red-staining granular deposits within the cytoplasm of hepatocytes (3)this is alcoholic hyalin. Alcoholic hyalin is easily distinguished from red blood cells (2) that are also present in this section.
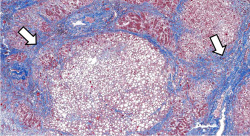
This is a low-power photomicrograph of liver stained with a trichrome stain. In this section, connective tissue stains blue (arrows) and hepatic parenchymal cells are red. Note that many of the parenchymal cells have clear spaces indicating fatty degeneration. The proliferation of scar tissue between the liver lobules is the result of cirrhosis.
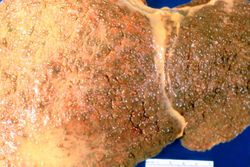
This gross photograph of liver demonstrates severe nodular cirrhosis. Note the extensive scarring of the capsule and the nodular projections of tissue through the uncut capsule in this tissue. The green color is due to the accumulation of bile pigment.

This is a cut surface of the same tissue seen in the previous slide. Note the marked nodular pattern. The paler-staining areas between the round nodules represent fibrous connective tissue.










Virtual Microscopy[edit]
Liver: Fatty Change and Cirrhosis[edit]
Normal Liver[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Cirrhosis
- eMedicine Medical Library: Alcoholic Hepatitis
- Merck Manual: Alcoholic Liver Disease
- Merck Manual: Cirrhosis
Journal Articles[edit]
- Satapathy SK, Narayan S, Varma N, Dhiman RK, Varma S, Chawla Y. Hyposplenism in alcoholic cirrhosis, facts or artifacts? A comparative analysis with non-alcoholic cirrhosis and extrahepatic portal venous obstruction. J Gastroenterol Hepatol 2001 Sep;16(9):1038-43.
Images[edit]
Related IPLab Cases[edit]
| |||||
A normal PaCO2 is 35 to 45 mmHg.
In alcoholics, aspiration pneumonia is common--bacteria enter the lung via aspiration of gastric contents.
Necrotizing lobar pneumonia is a severe acute pneumonia caused by virulent organisms and aspirated of gastric contents.
A normal liver weighs 1650 grams (range: 1500 to 1800 grams).
Cirrhosis is a liver disease characterized by necrosis, fibrosis, loss of normal liver architecture, and hyperplastic nodules.
Nodular hyperplasia of the prostate--characterized by large discrete prostatic nodules--is a common disorder in men over 50 years of age. The nodules cause the prostate to be enlarged and to have an increased weight. The human prostate is surrounded by a restrictive capsule. These nodules cause increased pressure within the capsule which leads to constriction of the urethra as it passes through the prostate. Urethral constriction leads to retention of urine.