Difference between revisions of "IPLab:Lab 6:Graves Disease"
Seung Park (talk | contribs) (Created page with "== Images == <gallery heights="250px" widths="250px"> File:IPLab6GravesDisease1.jpg|This is a photograph of the thyroid from this case. Note that the gland is enlarged and is ...") |
(→Images) |
||
| (15 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
| + | == Clinical Summary == | ||
| + | This 18-year-old girl presented with complaints of swelling in the neck, weight loss, bulging of the eyes, tremor, decreased heat tolerance, loose stools, and occasional palpitations. Physical examination revealed normal blood pressure, resting tachycardia of 110 beats per minute, mild exophthalmos, eyelid lag, and a diffusely enlarged thyroid gland. Pertinent laboratory findings were thyroxine (T4) level 30.8 mcg/dL, free thyroxine was 2.7 ng/dL , and thyroid stimulating hormone (TSH) was 0.22 mcIU/mL . She was given propylthiouracil until she became nearly euthyroid, at which time a thyroidectomy was done. The thyroid gland weighed 45 grams. It was beefy red in color and had a homogeneous fleshy consistency. | ||
| + | |||
== Images == | == Images == | ||
<gallery heights="250px" widths="250px"> | <gallery heights="250px" widths="250px"> | ||
| − | File: | + | File:IPLab6GravesDisease1b.jpg|This is a photograph of the thyroid from this case. Note that the gland is enlarged and is dark red. |
File:IPLab6GravesDisease2.jpg|This is a low-power photomicrograph of thyroid tissue from this case. The tissue is very cellular with very little colloid. | File:IPLab6GravesDisease2.jpg|This is a low-power photomicrograph of thyroid tissue from this case. The tissue is very cellular with very little colloid. | ||
| − | File: | + | File:IPLab6GravesDisease3x.jpg|This is a higher-power photomicrograph of thyroid. The tissue is very cellular and there is much less colloid (C) filling the glands than is normally seen. |
File:IPLab6GravesDisease4.jpg|This is a high-power photomicrograph of thyroid. Note the cellularity of the tissue with marked infolding of the epithelial tissue. | File:IPLab6GravesDisease4.jpg|This is a high-power photomicrograph of thyroid. Note the cellularity of the tissue with marked infolding of the epithelial tissue. | ||
| − | File: | + | File:IPLab6GravesDisease5x.jpg|This is a high-power photomicrograph of thyroid. Note the papillary projections and the “scalloped” or “moth-eaten” appearance (arrows) of the colloid (C). This appearance indicates active absorption of the colloid to form thyroglobulin. |
File:IPLab6GravesDisease6.jpg|This is a gross photograph of a thyroid from a case of nodular goiter. | File:IPLab6GravesDisease6.jpg|This is a gross photograph of a thyroid from a case of nodular goiter. | ||
| − | File: | + | File:IPLab6GravesDisease7b.jpg|Closer view of cut surface of the thyroid with nodular goiter. Note the multilobular appearance of the tissue. |
</gallery> | </gallery> | ||
| + | |||
| + | == Virtual Microscopy == | ||
| + | <peir-vm>IPLab6GravesDisease</peir-vm> | ||
| + | |||
| + | == Study Questions == | ||
| + | * <spoiler text="What is the immunologic mechanism responsible for Graves' disease?">Autoantibodies directed towards the TSH receptor of the thyroid cause stimulation of the thyroid leading to increased secretion of thyroid hormones and growth of the thyroid gland.</spoiler> | ||
| + | * <spoiler text="What role does genetics play in the predisposition to Graves' disease?">* Graves' disease is more common in females than males | ||
| + | * It has been linked to HLA-B8 and DR3 in whites but different haplotypes in Asians | ||
| + | * It has a familial predisposition | ||
| + | * It is more common in patients with other forms of autoimmune thyroid problems (e.g., Hashimoto's thyroiditis)</spoiler> | ||
| + | * <spoiler text="Does Graves' disease predispose to thyroid cancer?">There is little evidence to suggest an increased frequency of thyroid cancer in patients with Graves' disease.</spoiler> | ||
| + | |||
| + | == Additional Resources == | ||
| + | === Reference === | ||
| + | * [http://emedicine.medscape.com/article/920283-overview eMedicine Medical Library: Pediatric Graves Disease] | ||
| + | * [http://emedicine.medscape.com/article/767130-overview eMedicine Medical Library: Hyperthyroidism, Thyroid Storm, and Graves Disease] | ||
| + | * [http://emedicine.medscape.com/article/120034-overview eMedicine Medical Library: Goiter] | ||
| + | * [http://emedicine.medscape.com/article/120140-overview eMedicine Medical Library: Diffuse Toxic Goiter] | ||
| + | * [http://www.merckmanuals.com/professional/endocrine_and_metabolic_disorders/thyroid_disorders/overview_of_thyroid_function.html Merck Manual: Overview of Thyroid Function] | ||
| + | * [http://www.merckmanuals.com/professional/endocrine_and_metabolic_disorders/thyroid_disorders/hyperthyroidism.html Merck Manual: Hyperthyroidism] | ||
| + | |||
| + | === Journal Articles === | ||
| + | * Smith TJ and Hegedüs L. [http://www.nejm.org/doi/full/10.1056/NEJMra1510030 Graves’ Disease]. NEJM 2016 375:1552-1565. | ||
| + | * Fraser T, Green D. [http://www.ncbi.nlm.nih.gov/pubmed/11554873 Weathering the storm: beta-blockade and the potential for disaster in severe hyperthyroidism]. ''Emerg Med (Fremantle)'' 2001 Sep;13(3):376-80. | ||
| + | |||
| + | === Images === | ||
| + | * [{{SERVER}}/library/index.php?/tags/15-endocrine/140-thyroid/651-autoimmune_thyroiditis PEIR Digital Library: Autoimmune Thyroiditis Images] | ||
| + | * [http://library.med.utah.edu/WebPath/ENDOHTML/ENDOIDX.html Webpath: Endocrine Pathology] | ||
| + | |||
| + | == Related IPLab Cases == | ||
| + | * [[IPLab:Lab 6:Hashimoto's Thyroiditis|Lab 6: Thyroid: Hashimoto's Thyroiditis]] | ||
| + | * [[IPLab:Lab 7:Adenoma|Lab 7: Thyroid: Adenoma]] | ||
{{IPLab 6}} | {{IPLab 6}} | ||
[[Category: IPLab:Lab 6]] | [[Category: IPLab:Lab 6]] | ||
Latest revision as of 23:18, 8 July 2020
Contents
Clinical Summary[edit]
This 18-year-old girl presented with complaints of swelling in the neck, weight loss, bulging of the eyes, tremor, decreased heat tolerance, loose stools, and occasional palpitations. Physical examination revealed normal blood pressure, resting tachycardia of 110 beats per minute, mild exophthalmos, eyelid lag, and a diffusely enlarged thyroid gland. Pertinent laboratory findings were thyroxine (T4) level 30.8 mcg/dL, free thyroxine was 2.7 ng/dL , and thyroid stimulating hormone (TSH) was 0.22 mcIU/mL . She was given propylthiouracil until she became nearly euthyroid, at which time a thyroidectomy was done. The thyroid gland weighed 45 grams. It was beefy red in color and had a homogeneous fleshy consistency.
Images[edit]
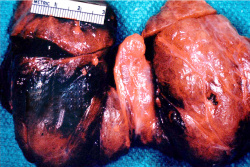
This is a photograph of the thyroid from this case. Note that the gland is enlarged and is dark red.
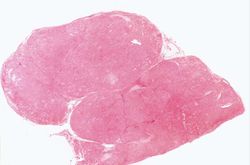
This is a low-power photomicrograph of thyroid tissue from this case. The tissue is very cellular with very little colloid.
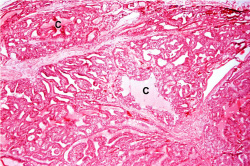
This is a higher-power photomicrograph of thyroid. The tissue is very cellular and there is much less colloid (C) filling the glands than is normally seen.
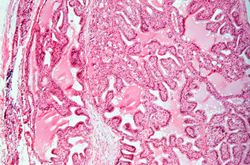
This is a high-power photomicrograph of thyroid. Note the cellularity of the tissue with marked infolding of the epithelial tissue.
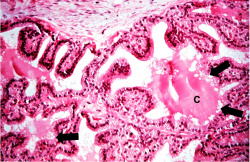
This is a high-power photomicrograph of thyroid. Note the papillary projections and the “scalloped” or “moth-eaten” appearance (arrows) of the colloid (C). This appearance indicates active absorption of the colloid to form thyroglobulin.

This is a gross photograph of a thyroid from a case of nodular goiter.
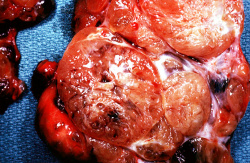
Closer view of cut surface of the thyroid with nodular goiter. Note the multilobular appearance of the tissue.







Virtual Microscopy[edit]
Study Questions[edit]
Additional Resources[edit]
Reference[edit]
- eMedicine Medical Library: Pediatric Graves Disease
- eMedicine Medical Library: Hyperthyroidism, Thyroid Storm, and Graves Disease
- eMedicine Medical Library: Goiter
- eMedicine Medical Library: Diffuse Toxic Goiter
- Merck Manual: Overview of Thyroid Function
- Merck Manual: Hyperthyroidism
Journal Articles[edit]
- Smith TJ and Hegedüs L. Graves’ Disease. NEJM 2016 375:1552-1565.
- Fraser T, Green D. Weathering the storm: beta-blockade and the potential for disaster in severe hyperthyroidism. Emerg Med (Fremantle) 2001 Sep;13(3):376-80.
Images[edit]
Related IPLab Cases[edit]
A normal T4 level is 4 to 11 mcg/dL.
A normal free T4 level is 0.71 to 1.85 ng/dL.
A normal thyroid gland weighs 25 grams.
Nodular hyperplasia of the prostate--characterized by large discrete prostatic nodules--is a common disorder in men over 50 years of age. The nodules cause the prostate to be enlarged and to have an increased weight. The human prostate is surrounded by a restrictive capsule. These nodules cause increased pressure within the capsule which leads to constriction of the urethra as it passes through the prostate. Urethral constriction leads to retention of urine.
Autoimmune disorders involve an immune response directed at the host's own cells.