Difference between revisions of "Cytologically Yours: CoW: 20131111"
(→Pathology) |
Seung Park (talk | contribs) m (1 revision) |
(No difference)
| |
Latest revision as of 19:29, 9 January 2014
Clinical Summary
The patient is an 80 year old male who presented to the Emergency Department with a chief complaint of right flank pain. He described the pain as a 10/10 pain in his right flank. He denied any associated symptoms with this pain. He denied constipation, cough, shortness of breath, fever, dysuria, hematuria, nausea, or diarrhea. He could not identify anything that made the pain worse or better. He did take 5mg of acetaminophen-hydrocodone and did not have any relief. He had just taken his evening medications when the pain began, and he can not identify any activity that may have caused the pain.
Past Medical History
- Chronic obstructive pulmonary disease
- Allergic rhinitis
- Hypertension
- Hyperlipidemia
- Diverticulosis
- Coronary artery disease
- Diabetes mellitus type 2
Past Surgical History
- 1993 Disk arthroplasty
- 2002 Coronary artery bypass with grafting
- 2009 arthroplasty
- Cholecystectomy year unknown
Medications
- Acetominophen-hydrocodone
- Acetaminophen-oxycodone
- Albuterol
- Aspirin
- Gabapentin
- Losartan
- Meloxicam
- Metoprolol
- Nitroglycerin
Clinical Plan
Differential diagnosis for flank pain includes: kidney stone, vertebral compression fracture,and infection. The suspicion for kidney stone was highest on the list. A urine culture, abdominal CT, and POC urine were ordered.
Radiology
CT scan revealed multiple lytic and sclerotic lesions within the thoracolumbar spine and sacrum. These were thought to be suspicious of metastatic disease. Wall thickening in the descending colon was seen and was thought to possibly represent a primary colon cancer. The prostate was enlarged.
The clinicians decided to perform a CT guided biopsy and a touch prep was made for rapid interpretation by the Cytology team.
CT



Pathology
Touch Preparation
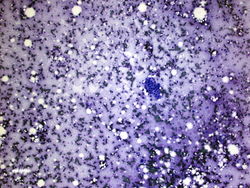
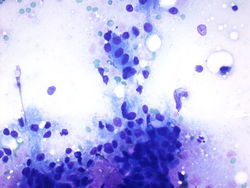
This is a 10x magnification the cytology specimen from the spinal mass. We see red blood cells and a cohesive group of cells in this field.
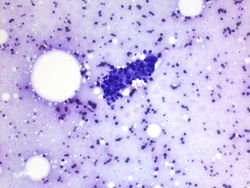
This is a 20x magnification of the cytology specimen from the spinal mass. We can see red blood cells in the background and a cohesive group of cells in this field.
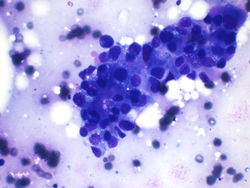
This is a 60x magnification of the cytology specimen from the spinal mass. We can see this group of cohesive cells have round nuclei, prominent nucleoli, and ample cytoplasm.
This is a 60x magnification of the cytology specimen from the spinal mass. Again we have a cohesive group of cells that have ample cytoplasm, round nuclei, and some prominent nucleoli.
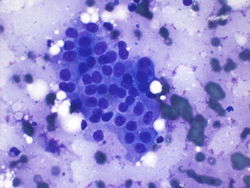
This is a 60x magnification of the cytology of the specimen from the spinal mass.
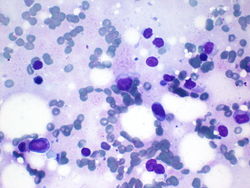
This is a 40x magnification of single cells in cytology specimen from the spinal mass. These single cells are much larger than the red blood cells, have ample cytoplasm, and are larger than the lymphocytes that are also present in the image.






Resident Questions
Biopsy
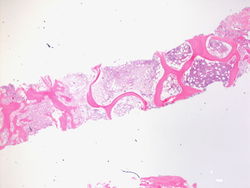
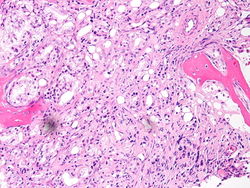
This is a 2x magnification the biopsy specimen from the spinal mass. We see that this is bone histology which is abnormal. There is an increase in cellularity, especially for an 80 year old person.
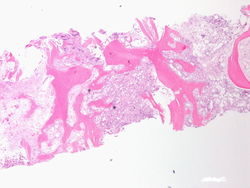
This is a 4x magnification of the biopsy specimen from the spinal mass. We can see that there is an increase in cellularity.
This is a 20x magnification of the biopsy specimen from the spinal mass. This is one of the areas that has increased cellularity on lower power. We can see cells forming what appear to be glands in the bone marrow.
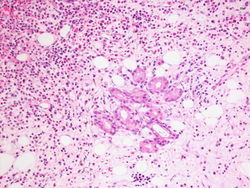
This is a 20x magnification of the biopsy specimen from the spinal mass. Here we see well formed glands in the bone marrow.
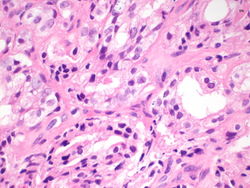
This is a 60x magnification of the biopsy specimen from the spinal mass. The malignant cells appear to be creating glandular structures, and we can identify prominent nucleoli in the malignant cells.
This is a 60x magnification of the biopsy specimen from the spinal mass. Again we see well formed glands in the bone marrow, made of cells that have prominent nucleoli.






Immunohistochemistry
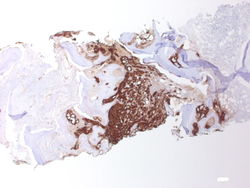
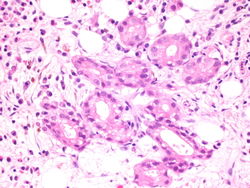
PSA, 2x magnification. Note the predominance of brown staining in the middle.
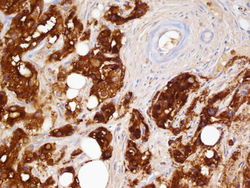
PSA, 60x magnification. The glands are highlighted in brown, and on the upper right the blood vessels are negative.


Resident Questions
Final Diagnosis
Cytology
- Positive for malignancy.
Biopsy
- Metastatic prostatic adenocarcinoma.
Case Discussion
This is a classic case of prostatic adenocarcinoma, metastatic to the spine.
| ||||||||