Difference between revisions of "IPLab:Lab 11:Ascariasis"
Seung Park (talk | contribs) |
Seung Park (talk | contribs) (→Images) |
||
| (5 intermediate revisions by the same user not shown) | |||
| Line 20: | Line 20: | ||
* <spoiler text="Was the original diagnosis of streptococcal pharyngitis in error? Does it relate to the subsequent intestinal obstruction?">The patient did have streptococcal pharyngitis. The high fever produced by the streptococcal infection "upset" the intestinal parasites and made them become more active and possibly contributed to the mass of worms that resulted in the intestinal obstruction.</spoiler> | * <spoiler text="Was the original diagnosis of streptococcal pharyngitis in error? Does it relate to the subsequent intestinal obstruction?">The patient did have streptococcal pharyngitis. The high fever produced by the streptococcal infection "upset" the intestinal parasites and made them become more active and possibly contributed to the mass of worms that resulted in the intestinal obstruction.</spoiler> | ||
* <spoiler text="How is ascariasis transmitted? How does this relate to the multiplicity of parasites identified in this patient's stool specimen?">Ascariasis and the two protozoan parasites seen in this woman are common in countries with poor sanitation. This can include fecal contamination of water, soil and therefore fruits and vegetables that are not washed adequately. After Ascaris eggs are excreted in the feces of the primary host, the eggs must incubate in soil for two weeks before they are infective. After two weeks, ingested embryonated eggs hatch and the larval worms burrow through the wall of the small intestine and enter the blood. They are primarily filtered out in the capillaries of the lung where they burrow into the alveoli, are coughed up and swallowed. They then take up residence in the small intestine. Children who practice geophagia commonly have very high Ascaris loads in areas with promiscuous defecation. The two protozoa form cysts in the colon of patients who do not have severe diarrhea and are infectious as soon as passed. The cysts remain viable in soil and water for weeks to months. The most likely common source for these three organisms would be non-chlorinated water or fruits and vegetables contaminated with soil or water. A food handler with Ascaris is not a public health threat while infection with either of the other organisms is a risk for transmission.</spoiler> | * <spoiler text="How is ascariasis transmitted? How does this relate to the multiplicity of parasites identified in this patient's stool specimen?">Ascariasis and the two protozoan parasites seen in this woman are common in countries with poor sanitation. This can include fecal contamination of water, soil and therefore fruits and vegetables that are not washed adequately. After Ascaris eggs are excreted in the feces of the primary host, the eggs must incubate in soil for two weeks before they are infective. After two weeks, ingested embryonated eggs hatch and the larval worms burrow through the wall of the small intestine and enter the blood. They are primarily filtered out in the capillaries of the lung where they burrow into the alveoli, are coughed up and swallowed. They then take up residence in the small intestine. Children who practice geophagia commonly have very high Ascaris loads in areas with promiscuous defecation. The two protozoa form cysts in the colon of patients who do not have severe diarrhea and are infectious as soon as passed. The cysts remain viable in soil and water for weeks to months. The most likely common source for these three organisms would be non-chlorinated water or fruits and vegetables contaminated with soil or water. A food handler with Ascaris is not a public health threat while infection with either of the other organisms is a risk for transmission.</spoiler> | ||
| + | |||
| + | == Additional Resources == | ||
| + | === Reference === | ||
| + | * [http://emedicine.medscape.com/article/212510-overview eMedicine Medical Library: Ascariasis] | ||
| + | * [http://www.merckmanuals.com/professional/infectious_diseases/nematodes_roundworms/ascariasis.html Merck Manual: Ascariasis] | ||
| + | |||
| + | === Journal Articles === | ||
| + | * ten Hove RJ, van Esbroeck M, Vervoort T, van den Ende J, van Lieshout L, Verweij JJ. [http://www.ncbi.nlm.nih.gov/pubmed/19415354 Molecular diagnostics of intestinal parasites in returning travellers]. ''Eur J Clin Microbiol Infect Dis'' 2009 Sep;28(9):1045-53. | ||
| + | |||
| + | === Images === | ||
| + | * [{{SERVER}}/library/index.php?/tags/2162-ascariasis PEIR Digital Library: Ascariasis] | ||
| + | * [http://library.med.utah.edu/WebPath/INFEHTML/INFECIDX.html WebPath: Infection] | ||
{{IPLab 11}} | {{IPLab 11}} | ||
[[Category: IPLab:Lab 11]] | [[Category: IPLab:Lab 11]] | ||
Latest revision as of 01:46, 30 August 2013
Contents
Clinical Summary[edit]
Shortly after arriving home after two years in Peru with the Peace Corps this 27-year-old female presented to the emergency room with a fever of 103.5°, anterior cervical lymphadenopathy, and pharyngitis. A rapid Strep test was positive and she was treated with penicillin.
Two days later she returned to the emergency room with abdominal distension, paroxysmal periumbilical pain, and repeated emesis. On examination, there was diffuse abdominal tenderness and bowel sounds were hyperactive and high-pitched. The WBC count was unremarkable except for a 12% eosinophilia. An upright film of the abdomen revealed dilated loops of small bowel with air fluid levels and the absence of colonic gas. Surgical exploration confirmed the presumptive diagnosis of small bowel obstruction and identified a tangled mass of approximately 50 adult Ascaris lumbricoides worms as the cause.
One-week post surgery, stool examination revealed the continued presence of Ascaris ova, as well as cysts of Entamoeba histolytica and Giardia lamblia. The patient was treated with appropriate anthelmintics and made a complete recovery.
Images[edit]

This is a photograph of an adult ascarid like the ones removed from the small bowel of this patient.

This is a photograph of an autopsy specimen from another case of ascariasis. The adult ascarid (arrow) can be seen in the section of small bowel from this patient.
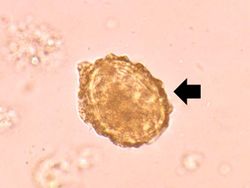
This is a high-power photomicrograph of a fecal specimen from this patient showing an ascarid egg (arrow).
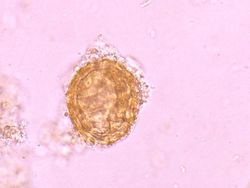
This is a higher-power photomicrograph of another ascarid egg.
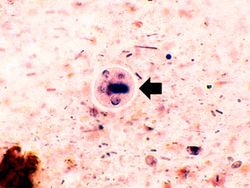
This high-power photomicrograph of the fecal specimen from this same patient shows an Entamoeba histolytica cyst (arrow).
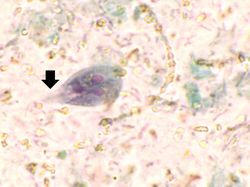
This high-power photomicrograph of the fecal specimen from this patient shows a Giardia lamblia trophozoite. Note the two nuclei and the tapered end (that goes out of the plane of focus) containing flagella (arrow).
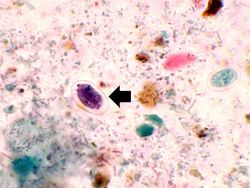
This high-power photomicrograph of the fecal specimen from this patient shows a Giardia lamblia cyst (arrow).







Study Questions[edit]
Additional Resources[edit]
Reference[edit]
Journal Articles[edit]
- ten Hove RJ, van Esbroeck M, Vervoort T, van den Ende J, van Lieshout L, Verweij JJ. Molecular diagnostics of intestinal parasites in returning travellers. Eur J Clin Microbiol Infect Dis 2009 Sep;28(9):1045-53.
Images[edit]
| |||||
A normal eosinophil count is less than 5%.